




Article
First Experiences Using Shimadzu's New "unity edition" Angiography System ―Kokura Memorial Hospital―
Kokura Memorial Hospital has started using one of Shimadzu's new "unity edition“ angiography systems. Kokura Memorial Hospital has used Shimadzu's angiography systems since becoming the first hospital in Japan to perform percutaneous coronary intervention (PCI) and up to the present day. We asked Dr. Kenji Ando (Consultant/Chief Director of the Department of Cardiology), Dr. Yoshimitsu Soga (General Manager of the Department of Cardiology), and Dr. Ryouji Ichinose (General Manager, Radiological Technologist) why Kokura Memorial Hospital, simultaneously a pioneer in cardiovascular medicine and a leader in the treatment for cardiovascular disease in Japan, continues to choose Shimadzu's systems and the appeal of Shimadzu's "unity edition."

Consultant/Chief Director of the Department of Cardiology

First, please tell us the history of Kokura Memorial Hospital, developments at the hospital, and the continuous presence of Shimadzu angiography systems during those times.
- Ando
- In 1974, after being assigned to the department of internal medicine at Kokura Memorial Hospital, Dr. Masakiyo Nobuyoshi* started to administer medical treatment focused on the circulatory system. Dr. Hideyuki Nosaka and Dr. Yukiyoshi Ito later joined Dr. Nobuyoshi, and established the Department of Cardiology in 1979. Catheter-based examinations began around this time, with PCIs beginning in 1981. According to Dr. Nobuyoshi, with the Department of Cardiology just established they were unable to procure an expensive angiography system, and instead performed cardiac catheterization using a Shimadzu gastric fluoroscopy system. This was apparently done because they were asked to perform cardiac catheterization by Dr. Toshihiko Ban* of the Department of Cardiovascular Surgery in order to perform bypass surgery. But they could not see any vessels using the gastric fluoroscopy system. I heard that because of this they carried out joint research with Shimadzu and improved the system into a cine film cardiac catheterization fluoroscopy system. I started working at Kokura Memorial Hospital in 1996, when cardiac catheterization was still performed with cine film and a manually operated C-arm. An electrically-operated C-arm was later introduced, and in around 2005 the hospital stopped using cine film and began moving towards digitalization. Since then, flat panels and a variety of other image processing technologies have been developed and improved image quality dramatically. Many patients were treated thanks to the work of Shimadzu, so I am very grateful to them.
* Now honorary directors

From the viewpoint of medical technology, tell us about the evolution of therapeutic technologies and the transition between Shimadzu angiography systems used at Kokura Memorial Hospital.
- Ichinose
- When I started working at Kokura Memorial Hospital, over 30 years ago, there were no satisfactory C-arm systems, so we collaborated with Shimadzu in developing a C-arm system for coronary artery interventions that resulted in them building a system unique to Kokura Memorial Hospital. It was a time of dramatic advancement in devices for coronary artery interventions, and all Japanese clinical trials of new devices that emerged in the 1990s were initially performed at Kokura Memorial Hospital. My impression of the time is that Shimadzu systems played a significant role in this work.
The biggest change that has occurred in systems since that time, and the biggest achievement in our eyes, has been flat panels. All the manufacturers of the time experienced great difficulty, and I remember having tremendous problems with Shimadzu's first version of their flat panel. As we discussed with Shimadzu how to deal with image noise and power supplies for flat panels, Shimadzu made modifications and their systems changed little by little before our eyes. Of prime concern at the time was how flat panels could be used in clinical practice, and how we and Shimadzu could convince Dr. Nobuyoshi about the technology.
After advancements in flat panels slowed down a little, PCI-specific applications were the next area to see development. Advances were being made in all devices including the struts of drug-eluting stent (DES). These became thinner, which also worsened their visibility. Applications designed to improve stent visibility appeared for non-Shimadzu systems, but these applications performed image processing very slowly and only produced still images. Asking at other medical facilities, almost all would tell us they did not use these applications.
Then Shimadzu developed a real-time application called StentView, which lead to increased interest in the topic of applications that enhanced stent visibility. I am almost certain StentView's popularity was due to its real-time performance. After all, cardiac medicine is a race against time.
And now, Kokura Memorial Hospital also performs arrhythmia treatment and endovascular treatment (EVT).
- Ando
- It does. Of course, at first, we only performed contrast-enhanced imaging of the coronary artery and bypass treatment. We also performed ergonovine stimulation testing with drug therapy, but PCIs started in 1981. After that, bare-metal stent treatment began in the 1990s, and ablations and EVT became more common in the mid-2000s. This prompted in ablation a need for bi-plane systems instead of single-plane systems, and in EVT a need for dedicated contrast enhanced imaging of the legs. I believe these changes are what precipitated the development of systems capable in a variety of fields, and not just for the imaging of coronary arteries.
What role did Shimadzu angiography systems play amongst all this?
- Soga
- Apart from the heart, ablations and EVT also emerged as mainstays of medical care services at Kokura Memorial Hospital. This came with the need for a single system capable of performing in multiple roles. We previously used a system designed for Yoshimitsu Soga, General Manager of the Department of Cardiology Ryouji Ichinose, General Manager, Radiological Technologist No.83 (2018.3) coronary arteries for lower extremity imaging, but this system limited the range of services we could provide. Also, using a system designed for cardiac imaging did not produce satisfactory image quality when used for the intestines and the legs, which are longer target regions compared to the heart. Since then, Shimadzu has done great work in improving in these areas.
If I was to speak frankly about what I liked about Shimadzu, it was they came right away when called. Being a domestic Japanese manufacturer, they are quick to respond to inquiries. They are also prepared to make changes to even minor things, and I think the high quality images they achieve today is thanks to making these kinds of ongoing minor improvements.
What are your thoughts on the reliability of Shimadzu systems and after-sales services?
- Soga
- I have heard about X-ray tubes suddenly cutting out at other hospitals, but that has never happened with our equipment despite the heavy load we put them under.
- Ando
- And our systems are in almost constant use every single day. But, if by chance something should go wrong, a service engineer will come the next day to carry out repairs.
- Ichinose
- Shimadzu has always been that way. As a rule, Shimadzu systems do not break down. They are also quick to start up, which is extremely important in emergency situations. It really helps. Shimadzu's "reBORN" has seen a substantial upgrade of Shimadzu systems in terms of system design, applications, and operability that are equivalent to introducing new products, which has also been very good for the user from a cost standpoint.
How is image quality with Shimadzu systems?
- Soga
- As I mentioned earlier, image quality has really improved with all the ongoing minor improvements. Overlapping of the intestinal tract and blood vessels dilutes the color of contrast media, and can sometimes make it difficult to tell if narrowing is present. But in these cases, narrowing has been made easier to assess thanks to increased performance in image outline and sharpening. Imaging of coronary arteries has also improved.
- Ando
- Before, I sometimes felt that wires were difficult to distinguish, but this has changed for the better now. Outlines are sharp, edges are defined, images are improved.
You recently obtained a "reBORN" package upgrade to the 16 × 12 inch field-of-view C16 unity edition. How is that performing?
- Soga
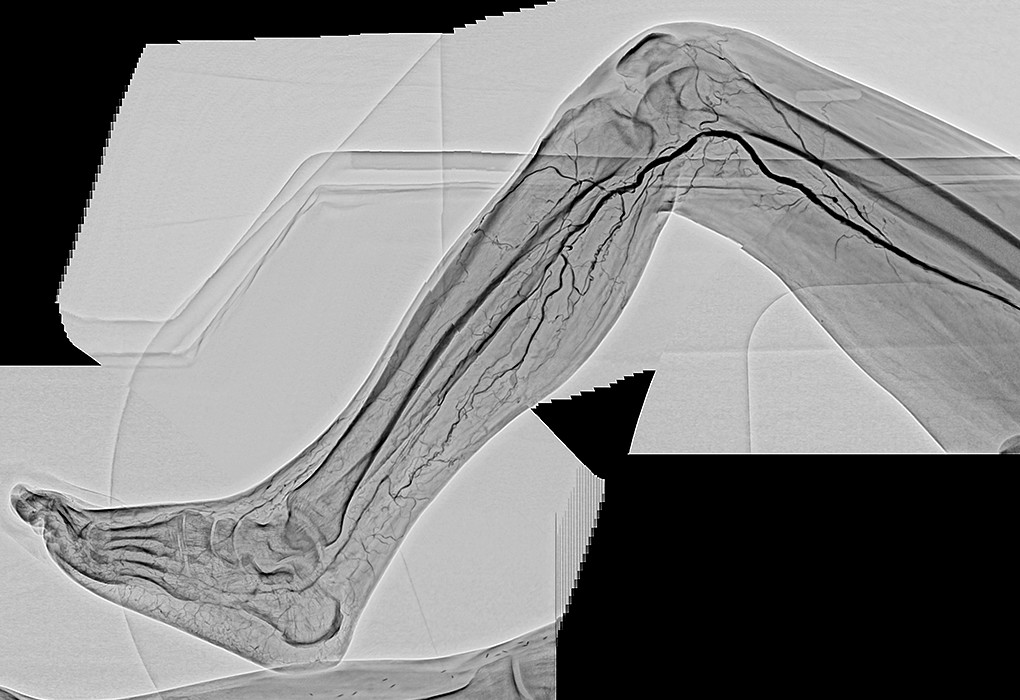
- First off, having both legs shown in a single image is very useful. We can also choose to use the 16-inch side in portrait or landscape orientation during procedure. For example, landscape is used when we want to view the entire length of both legs during tracking imaging. Before, digital subtraction angiography (DSA) was performed over a number of different acquisitions that increased the amount of contrast media used in the patient. Therefore, reducing the number of acquisitions has been a substantial benefit for patients. Of course, this would mean nothing if the system could not acquire satisfactory images of coronary arteries, but the system remains capable of acquiring coronary artery images as normal. The 16 × 12 inch panel also covers the entire region of interest during bypass surgery, so imaging is made easier with no need for tracking and no associated image blurring.
- Ichinose
- Panel size has increased, but the design has also been made cleaner and more compact making it more versatile. Also, as Dr. Soga mentioned, using the 16-inch side in landscape orientation lets us view the entire length of the lower extremities in a single acquisition during tracking imaging, but the table also has a long range of motion in a longitudinal direction that allows us to acquire images to the toes just by moving the table. Another notable upgrade is the new tilt function on the table, which I think we can use in the future depending on the application. Touch panels have also been added tableside in the examination room and in the control room that are extremely easy to use and have customizable functions.


How does the SCORE Chase application perform in assisting EVT?
- Ando
- SCORE Chase is good. It is amazing how it automatically follows vessels even when moving the table in a transverse direction. It makes me wonder why this application was not available earlier. All the visitors at our hospital have been surprised when they saw it.
- Soga
- Everyone remarks on how good it is. We used to connect images of blood vessels manually, which was hard work since brightness varied between images. That work has been made unnecessary thanks to SCORE Chase. The way it automatically adjusts the image and instantaneously connects it to other images is very useful.
- Ando
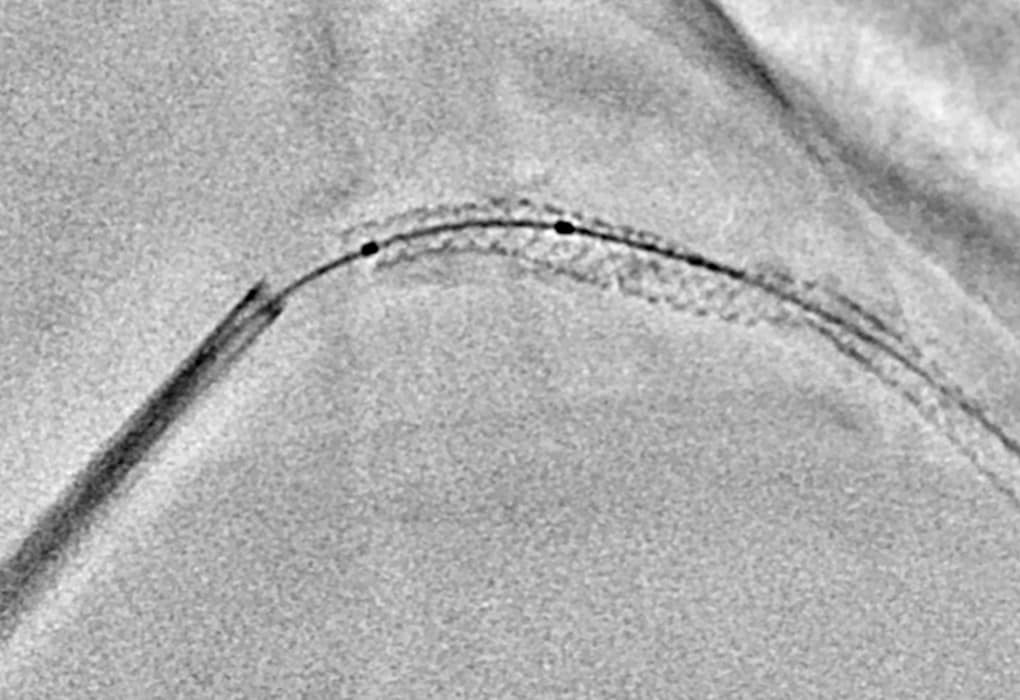
- We can see when there is poor stent dilation and each single strut of the stent. The narrow areas are shown clearly.
- Ichinose
- Another very good feature is when multiple devices are used, StentView has a function that allows us to set regions of interest to tell the application where to detect device markers. It takes a little time to get used to, but once you do it is very easy to use. Setting regions of interest is very effective for segments 1 and 2 of the right coronary artery, which moves a lot during cardiac motion, and it allows us to acquire demonstrably better images.
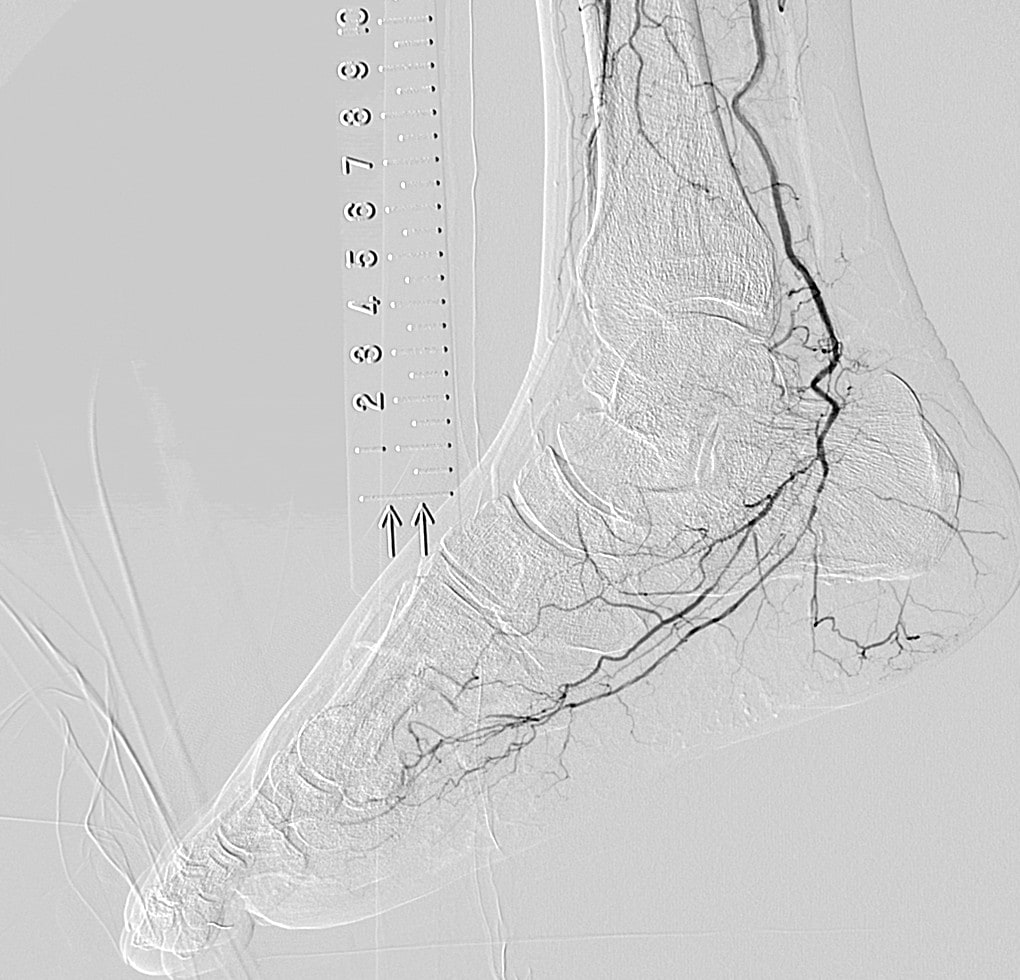
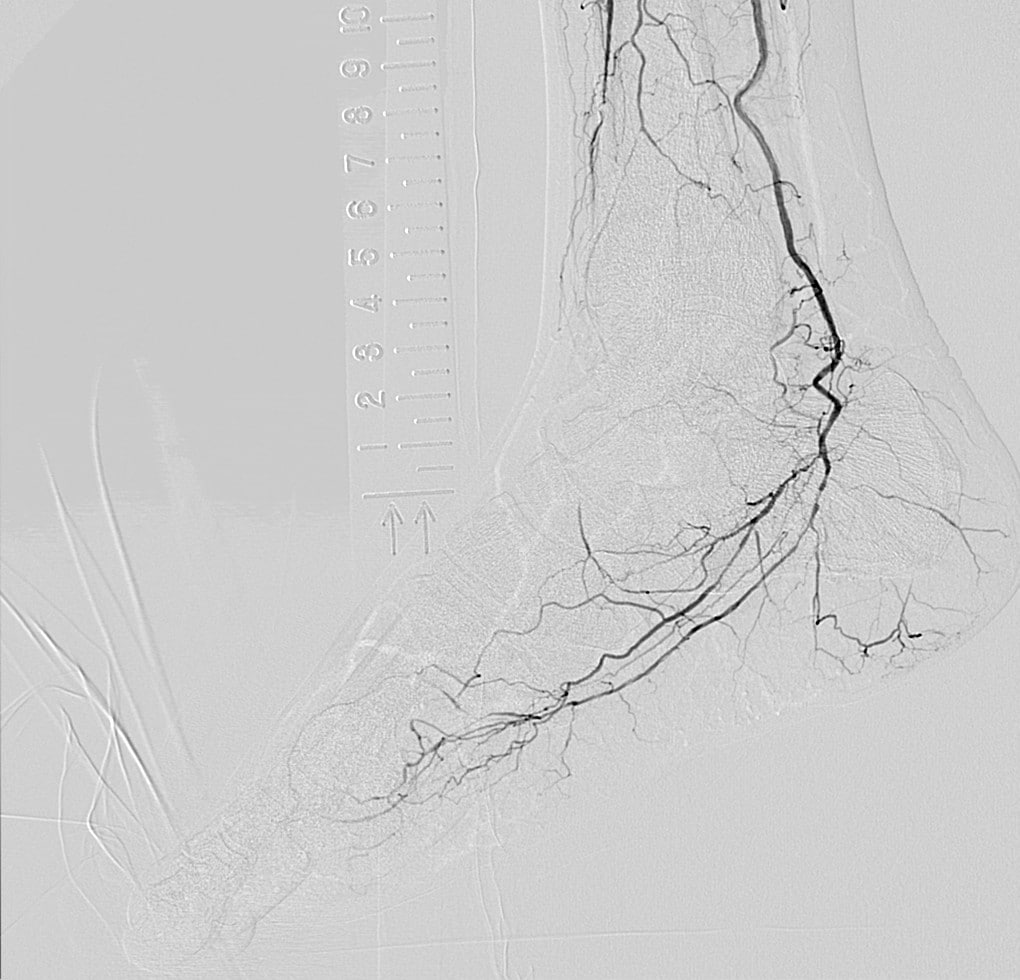
How is Flex-APS, which gives real-time correction of three-dimensional movement during DSA?
- Soga
- The margins of blood vessels are clearer now since it automatically processes images to correct for small subject movements and body vibrations.
- Ichinose
- I agree, Flex-APS is very good. Since it is always automatically correcting images for us, we have come to expect clear DSA images without misregistration artifacts. I have no complaints about usability at all, and feel it is suited to image acquisition for peripheral blood vessels.
Finally, could you speak on what you would like to see in the future from Shimadzu?
- Ando
- Shimadzu is actually meeting all our expectations. As a domestic Japanese company, I would like to see it develop even better products and applications to compete with foreign companies.
- Soga
- Shimadzu's products represent Japanese quality. Like a Toyota car they run without maintenance for more than 10 years, give good image quality, and come with other additional benefits. These features make up for the high initial investment.
- Ichinose
- As Dr. Ando and Dr. Soga have said, I would like to see Shimadzu focus on their strengths as a domestic Japanese manufacturer. There are some peculiarities in how equipment is used in Japan that Shimadzu should be quicker to understand. In terms of operability, the simpler it is the easier it is to use, and Shimadzu systems are certainly easy to operate, which I think is a result of Japanese ingenuity. I look forward to seeing more unique ideas like SCORE RSM that stop me in my tracks. Otherwise, compatibility with peripheral equipment. These days, we have an ever increasing amount of peripheral equipment, and compatibility with IVUS and other techniques will become a requirement.
- Ando
- In the future, I would like to see Shimadzu spread its wings around the world. I look forward to great things.